
Hypokalemia (K+ <2.5)
- ECG stat to look for hypokalemic changes
- 1g KCLin 100cc NS over 2hour (according to K+ level0 with continous cardiac monitoring
- add KCL in drip if any, mist KCL 15mls TDS/t slow K 600mg/1.2g OD
- off K supplements once K>4
- repeat 1 hour post correction
- Repeat cm?
ECG changes in Hypokalemia
- Increased amplitude and width of the P wave
- Prolongation of the PR interval
- T wave flattening and inversion
- ST depression
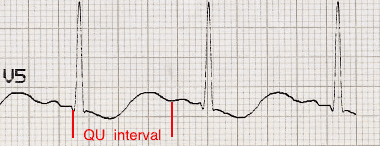
- Prominent U waves (best seen in the precordial leads)
- Apparent long QT interval due to fusion of the T and U waves (= long QU interval)
With worsening hypokalaemia…
- Frequent supraventricular and ventricular ectopics
- Supraventricular tachyarrhythmias: AF, atrial flutter, atrial tachycardia
- Potential to develop life-threatening ventricular arrhythmias, e.g. VT, VF and Torsades de Pointes


Handy tips
- Hypokalaemia is often associated with hypomagnesaemia, which increases the risk of malignant ventricular arrhythmias
- Check potassium and magnesium in any patient with an arrhythmia
- Top up the potassium to 4.0-4.5 mmol/l and the magnesium to > 1.0 mmol/l to stabilise the myocardium and protect against arrhythmias – this is standard practice in most CCUs and ICUs
Hyperkalemia (K+ >5.5)
- ECG stat to look for hyperkalemic changes
- off K supplements
- 10cc of 10% calcium gluconate in 10 minutes with cardiac monitoring + 50cc d50% glucose + 10 unit actrapid
- t kalimate 5-10g TDS
- off kalimate once K <5
- repeat 1 hour post chase
- repeat cm?
ECG manifestations in hyperkalaemia
- Peaked T waves
- Prolonged PR segment
- Loss of P waves
- Bizarre QRS complexes
- Sine wave
Effects of hyperkalaemia on the ECG
Serum potassium > 5.5 mEq/L is associated with repolarization abnormalities:
- Peaked T waves (usually the earliest sign of hyperkalaemia)
Serum potassium > 6.5 mEq/L is associated with progressive paralysis of the atria:
- P wave widens and flattens
- PR segment lengthens
- P waves eventually disappear
Serum potassium > 7.0 mEq/L is associated with conduction abnormalities and bradycardia:
- Prolonged QRS interval with bizarre QRS morphology
- High-grade AV block with slow junctional and ventricular escape rhythms
- Any kind of conduction block (bundle branch blocks, fascicular blocks)
- Sinus bradycardia or slow AF
- Development of a sine wave appearance (a pre-terminal rhythm)
Serum potassium level of > 9.0 mEq/L causes cardiac arrest due to:
- Asystole
- Ventricular fibrillation
- PEA with bizarre, wide complex rhythm

Handy Tips
Suspect hyperkalaemia in any patient with a new bradyarrhythmia or AV block, especially patients with renal failure, on haemodialysis or taking any combination of ACE inhibitors, potassium-sparing diuretics and potassium supplements.
credit: Life in the fast lane ECG and sources from study crew
