postpartum family planning aims to prevent unintended pregnancy and closely spaced pregnancies after childbirth
Method
Long acting reversible contraceptions (fit and forget) – most effective
IUD
Implant
hormonal contraception
COCP – combined oral contraceptive pill
POCP- progestogen- only contraceptive pill
Depo provera injection
barrier method
condoms – also protect against STI
internal condom –
emergency contraception
emergency contraceptive pill
copper IUD – (recommended if weight >70kg)
fertility awareness
calendar method
permanent contraception – most effective
vasectomy
tubal ligation
Long acting reversible contraceptions
IUD – Intrauterine Device
can start within 48 hours/ delayed after 4 weeks postpartum
prevent pregnancy for 5-10 years
eg; levonorgestrel – releasing IUD (Mirena) – up to 7 years
failure rates ; 1 in 1000 (0.001)
copper IUD does not interfere breastfeeding
return of fertility: immediate
side effect;
IUD may came out of uterus
infection
injury
hormonal IUD (mirena) cause spotting and irregular bleeding in first 3-6 months of use, headache, nausea, depression, breast tenderness
copper IUD increase menstrual pain and bleeding, intermenstrual bleeding. decrease within 1 year of use
Implants
release progestin
can start anytime
prevent pregnancy for 3-5 years
failure rates ; 1 in 1000 (0.001)
return of fertility: immediate
does not interfere breastfeeding
side effect;
irregular menses, intermenstural bleeding
mood changes
headache
acne
depression
Permanent Contraception
Female Sterilisation
can start within 7 days / after 6 weeks postpartum
failure rates ; 2 in 1000 (0.002)
Vasectomy
can start anytime
failure rates ; 1 in 1000 (0.001)
takes about 2 to 4 months for the semen to become totally free of sperm after a vasectomy. A couple must use another method of birth control or avoid sexual intercourse until a sperm count confirms that no sperm are present.
pros;
permanent birth control
no daily attention require
does not affect sexual pleasure
cons;
may regret
require surgery
may not be reversible
Hormonal contraception-
Progestogen – only injectable contraceptives (Depoprovera)
prevent pregnancy for 8-12 weeks ( 3 months )
can start anytime
failure rates ; 3 in 100 (0.03)
side effects: amenorrhea
return of fertility: months
does not interfere breastfeeding
side effect;
bone loss
irregular menses
headache
slight weight gain
Progestogen – only pills (POP)
contained progestin
taken continuously every day without a break
can start anytime
failure rates; 9 in 100 (0.09)
does not interfere breastfeeding
must be taken at the exact same time each day. If you miss a pill by more than 3 hours, you will need to use a back-up method for the next 48 hours.
benefit; reduce menstrual bleeding or stop period altogether
side effect
headache
nausea
breast tenderness
increase risk of breast ca
Combined oral contraceptive (COC) pills
contained progestin and estrogen
taken daily for 21 days followed by 7 days break when withdrawal bleeding ( menstruation) occurs
failure rates; 9 in 100 (0.09)
other form of COC – patch, vaginal ring
benefit;
regular, lighter, shorter menses
reduce cramps
improve acne
reduce menstrual migraine frequency
reduce unwanted hair growth
if women not breastfeeding, may start after 3 weeks postpartum unless they have rick of VTE, in which should only start COC after 6 weeks postpartum
side effect;
postpartum DVT
interfere with breastfeeding – should not be used by breastfeeding women until baby is 6 months old
risk of stroke and heart attacks ( not recommended in >35 years old, smoker, HPT, DM, stroke, breast ca)
breakthrough bleeding, headache, breast tenderness, nausea
Barrier method
spermicide
prevent transmission of gonorrhea and chlamydia.
It can be stored for long periods of time.
It may be messy, cause mild discomfort or minor allergic reaction, and can lead to yeast infections.
may cause vaginal irritation with frequent use
diaphragm
cervical cap
condoms
can use anytime
failure rates; 12 in 100 (0.12)
protect against STD
does not interfere breatsfeeding
cons
not suitable for pt with allergy to latex
interrupt sexual activity and may reduce sensation
withdrawal
can use anytime
failure rates; 18 in 100 (0.18)
does not interfere breatsfeeding
fertility awareness based methods (FAB)
can use anytime
failure rates; 24 in 100 (0.24)
not recommended post partum until women have regular menses for 3-4 cycles
Lactational amenorrhea method (LAM)
temporary method of birth control based on the natural way the body prevents ovulation when a woman is breastfeeding. It requires exclusive, frequent breastfeeding. The time between feedings should not be longer than 4 hours during the day or 6 hours at night. LAM may not be practical for many women.
emergency contraception
levonorgestrel (LNG) emergency contraception can be used anytime postpartum regardless of whether or not a woman is breastfeeding
high dose ethinyl estradiol either alone or in combination with progestogen (COCP) should not be used post partum due to risk of VTE
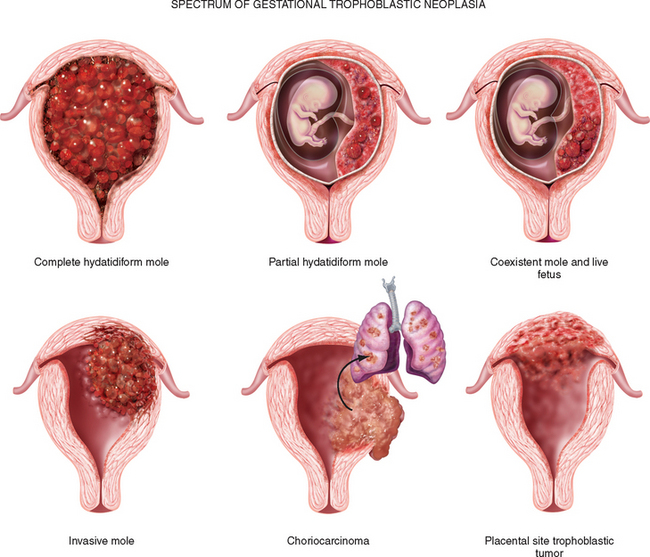
Gestational trophoblastic disease (GTD) is a group of rare tumors that involve abnormal growth of cells inside a woman’s uterus. GTD does not develop from cells of the uterus like cervical cancer or endometrial (uterine lining) cancer do. Instead, these tumors start in the cells that would normally develop into the placenta during pregnancy. (The term gestationalrefers to pregnancy.)
Types of gestational trophoblastic disease
Hydatidiform mole (complete or partial)
Invasive mole
Choriocarcinoma
Placental-site trophoblastic tumor
Epithelioid trophoblastic tumor
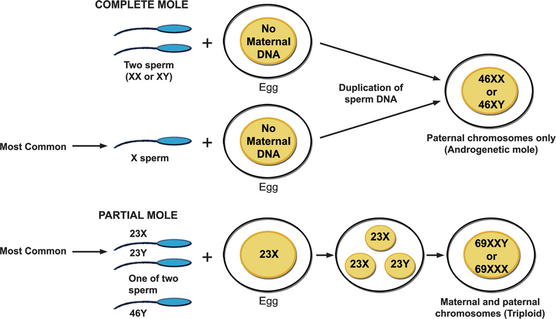
Normally, at fertilization, a single egg with 23 chromosomes fuses with a single sperm with 23 chromosomes, resulting in a new organism with 46 chromosomes. This can go wrong in two ways, so we have two kinds of moles – complete, or classic, and incomplete, or partial mole. Both lead to an abnormal proliferation of placental cells, and an abnormal placenta.
Complete mole appears when a chromosomally empty egg fuses with a normal sperm, and the sperm genetic material duplicates to form a 46 chromosome organism. However, this organism doesn’t have both maternal and paternal chromosomes, so the mole develops into a mass rather than developing into a fetus.
With a complete mole, the placenta secretes a huge amount of HCG. So affected females present with signs of pregnancy, like missed periods, and a positive urine pregnancy test.
Incomplete mole, on the other hand, appears when a normal egg is fertilized by two sperm – which forms an organism with 69 chromosomes, that usually develops into non-viable fetal parts.
Invasive mole (formerly known as chorioadenoma destruens) is a hydatidiform mole that has grown into the muscle layer of the uterus. Invasive moles can develop from either complete or partial moles, but complete moles become invasive much more often than do partial moles. Invasive moles develop in less than 1 out of 5 women who have had a complete mole removed. The risk of developing an invasive mole in these women increases if:
There is a long time (more than 4 months) between their last menstrual period and treatment.
The uterus has become very large.
The woman is older than 40 years.
The woman has had gestational trophoblastic disease in the past.
Choriocarcinoma is a malignant form of gestational trophoblastic disease (GTD). It is much more likely than other types of GTD to grow quickly and spread to organs away from the uterus.
Placental-site trophoblastic tumor (PSTT) is a very rare form of GTDthat develops where the placenta attaches to the lining of the uterus. This tumor most often develops after a normal pregnancy or abortion, but it may also develop after a complete or partial mole is removed.
Most PSTTs do not spread to other sites in the body. But these tumors have a tendency to grow into (invade) the muscle layer of the uterus.
Most forms of GTD are very sensitive to chemotherapy drugs, but PSTTs are not. Instead, they are treated with surgery, to completely remove disease.
Signs and symptoms
irregular vaginal bleeding range from light spotting to heavy bleeding, and parts of the mole may even be eliminated, and they look like grapes, or cherry-like clusters.
hyperemesis (due to huge amount of HCG)
excessive uterine enlargement
early failed pregnancy.
urine pregnancy test in women presenting with such symptoms.
physical examination shows a uterus that’s too big for gestational age since the mole grows much faster than a normal pregnancy would.
Rarer presentations in complete hydatidiform (high HCG level) include hyperthyroidism, early onset pre-eclampsia or abdominal distension due to theca lutein cysts. HCG has a subunit that’s similar to TSH, FSH, and LH. This causes symptoms of hyperthyroidism – like insomnia, anxiety, tachycardia, and palpitations, as well as the formation of theca lutein cysts on the ovaries, which can cause adnexal mass symptoms like pain or pressure on the affected side.
Very rarely, women can present with acute respiratory failure or neurological symptoms such as seizures; these are likely to be due to metastatic disease.
Diagnosis
ultrasound diagnosis of a partial molar pregnancy is more complex; the finding of multiple soft markers, including both cystic spaces in the placenta and a ratio of transverse to anterioposterior dimension of the gestation sac of greater than 1.5, is required for the reliable diagnosis of a partial molar pregnancy.
Estimation of hCG levels may be of value in diagnosing molar pregnancies: hCG levels greater than two multiples of the median may help.
*AM REVIEW must be complete and up to date with the progress*
B/O NORA / 32 HOURS OF LIFE (if more than 72 hours, just put how many days of life)
DOB: 1/8/2019 @ 3.30AM
SVD @ 39 weeks 2 days (if EMLSCS or ELLSCS, also state the reason – for suspicious CTG)
BW: 3.2 kg
CW: 3.0 kg (reduce 6.25%) – its normal for the baby to reduce in weight by 10-15% for the first 7-10 days then they will gain weight again. so if the weight reduce from 3.2 to 2.9 then up again to 3.0, dont state reduce. instead state increase using the difference between 2.9 and 3.0.
Apgar Score: 9/9
Liquor: clear/MMSL/LMSL
G6PD: normal or deficient – (only discharge baby if result of G6PD came out normal. if deficient, admit baby for 5 days for observation)
CTSH: normal is less than 21mIU/L
mother / 25 years old/ Para 2
Mother Blood Group – (if O+ve – think of ABO incompatibility in baby with jaundice onset less than 24 hours)
HIV/VDRL: Nonreactive
ANC:
GBS Carrier (find out more about the risk)
low risk – mother received IV C-penicillin 2 doses more than 4 hours prior to delivery
moderate risk – mother received only 1 doses of IV C-penicillin less than 4 hours prior to delivery
high risk – no antibiotic given
any maternal risk- maternal pyrexia-maternal UTI
ARM for how many hours prior to delivery. PROM more than 18 hours is a risk factor for sepsis
GDM on insulin
total insulin : 74 unit
latest HbA1c: 5.4% ( important to find out the glucose control. if uncontrol, baby had more risk of having hypoglycemia)
Single Parent
was referred to JKSP
if underage- referred to Pelindung, but still under JKSP
any other social issue
Issue:
Neonatal Jaundice
noted at how many hours of life.
noted by whom. JM visiting?
any TSB taken, Reticulocyte count
TSB @ 23 HOL : 234 (PL, ET)
TSB trend. take note of any respecification of the risk
feeding history:
exclusive breastfeeding / mixed feeding if breastfeeding – how long each session, whats the frequency (sustained 30mins – 45 mins each session, every 2-3 hours)
good latching, good letdown, good suckling
if mixed feeding – type of formula, dilution- how many scoop for how many ounces, frequency and amount
no traditional medicine or goats milk consumption
Infant of GDM mother on insulin
any jittery. any hypoglycemic symptom
reflo stable or not. less than 3 not stable
Failure to thrive
Infant of GBS carrier mother
on IV C-penicillin Day 2 and IV gentamicin Day 3 – to complete for 72 hours (must state abx on what day)
any sign of sepsis
TWC, Plt
Blood C+S
Progress/Currently:
tolerating feeding well
saturating well under room air
HR BP stable
Temp stable
PU BO normal
under single/double phototherapy
o/e: active, anterior fontanelle normotensive (AFNT), not tachypneic, CRT<2s, warm peripheries, good pulse volume,
lungs: clear
CVS: S1S2
PA: soft, not distended
Investigation
if on double photo, take TSB 4 hourly. if single photo, only take coming morning
if NNJ < 4 hours, suspect ABO. take ABO workup. BBG, FBC, Retics, Coombs
if presumed sepsis, take blood C+S
if on gentamicin, take renal profile post genta
Plan
Feeding – if on single photo – topup 10%. if double photo- topup 20%
1g KCLin 100cc NS over 2hour (according to K+ level0 with continous cardiac monitoring
add KCL in drip if any, mist KCL 15mls TDS/t slow K 600mg/1.2g OD
off K supplements once K>4
repeat 1 hour post correction
Repeat cm?
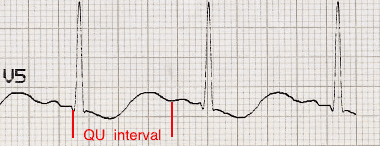
ECG changes in Hypokalemia
Increased amplitude and width of the P wave
Prolongation of the PR interval
T wave flattening and inversion
ST depression
Prominent U waves (best seen in the precordial leads)
Apparent long QT interval due to fusion of the T and U waves (= long QU interval)
With worsening hypokalaemia…
Frequent supraventricular and ventricular ectopics
Supraventricular tachyarrhythmias: AF, atrial flutter, atrial tachycardia
Potential to develop life-threatening ventricular arrhythmias, e.g. VT, VF and Torsades de Pointes
Handy tips
Hypokalaemia is often associated with hypomagnesaemia, which increases the risk of malignant ventricular arrhythmias
Check potassium and magnesium in any patient with an arrhythmia
Top up the potassium to 4.0-4.5 mmol/l and the magnesium to > 1.0 mmol/l to stabilise the myocardium and protect against arrhythmias – this is standard practice in most CCUs and ICUs
Hyperkalemia (K+ >5.5)
ECG stat to look for hyperkalemic changes
off K supplements
10cc of 10% calcium gluconate in 10 minutes with cardiac monitoring + 50cc d50% glucose + 10 unit actrapid
t kalimate 5-10g TDS
off kalimate once K <5
repeat 1 hour post chase
repeat cm?
ECG manifestations in hyperkalaemia
Peaked T waves
Prolonged PR segment
Loss of P waves
Bizarre QRS complexes
Sine wave
Effects of hyperkalaemia on the ECG
Serum potassium > 5.5 mEq/L is associated with repolarization abnormalities:
Peaked T waves (usually the earliest sign of hyperkalaemia)
Serum potassium > 6.5 mEq/L is associated with progressive paralysis of the atria:
P wave widens and flattens
PR segment lengthens
P waves eventually disappear
Serum potassium > 7.0 mEq/L is associated with conduction abnormalities and bradycardia:
Prolonged QRS interval with bizarre QRS morphology
High-grade AV block with slow junctional and ventricular escape rhythms
Any kind of conduction block (bundle branch blocks, fascicular blocks)
Sinus bradycardia or slow AF
Development of a sine wave appearance (a pre-terminal rhythm)
Serum potassium level of > 9.0 mEq/L causes cardiac arrest due to:
Asystole
Ventricular fibrillation
PEA with bizarre, wide complex rhythm
Handy Tips
Suspect hyperkalaemia in any patient with a new bradyarrhythmia or AV block, especially patients with renal failure, on haemodialysis or taking any combination of ACE inhibitors, potassium-sparing diuretics and potassium supplements.
credit: Life in the fast lane ECG and sources from study crew
PFANNESTIAL INCISION MADE AND ABDOMEN OPENED IN LAYERS
UV FOLD IDENTIFIED AND SEPARATED
BLADDER PUSHED AWAY CAUDALLY AND RETRACTED INFERIORLY WITH DOYAN’S RETRACTOR.
TRANSVERSE INCISION MADE AT LOWER SEGMENT OF UTERUS.
INCISION EXTENDED WITH BLUNT DISSECTION
AMNIOTOMY DONE AND BABY DELIVERED
PLACENTA AND MEMBRANES DELIVERED VIA CCT.
UTERUS CLOSED IN 2 LAYERS WITH VICRYL 1-0
FALLOPIAN TUBES AND OVARIES NORMAL
HAEMOSTASIS SECURED.
SWAB AND INSTRUMENT COUNTS WERE CORRECT.
RECTUS SHEATH WAS CLOSED WITH VICRYL 1.
SKIN WAS CLOSED VICRYL 2-0.
VAGINAL TOILET DONE AND BLOOD CLOTS EVACUATED.
POST OPERATIVE MANAGEMENT
TRANSFER OUT TO WARD ONCE PATIENT STABLE.
ALLOW ORALLY
LIE IN SUPINE POSITION FOR 6 HOURS (SPINAL)
BP/ PR MONITORING 1/4HOURLY UNTIL STABLE
CBD FOR ONE DAY
STRICT PAD CHARTING.
IVD 5 PINTS OF NSD5% / 24 H UNTIL PATIENT TAKING ORALLY WELL
CONTINUE ANALGESIA AS ORDERED BY ANESTHETIST. EG: SERVE SUP VOLTAREN 75MG BD. START FIRST DOSE 6 HOURS POST OP
SC HEPARIN 5000U BD TILL AMBULATING WELL
IV CEFOBID 1G BD + IV METRONIDAZSOLE 500MG TDS X 24 HOURS
WI DAY 2.
STO NOT REQUIRED
MODE OF DELIVERY NEXT PREGNANCY: TOS/LSCS
FBC DAY 2
IV PITOCIN 40U FOR 6H
Post Caesarian-section REVIEW
Age/race Para 1, Post ELLSCS 2 hours for breech presentation
ANC: Breech presentation with oligohydromnios
Intra operative findings: from op notes
Progress: Patient complains of minimal pain at the op site Otherwise: No dizziness/headache, No SOB/chest pain No palpitations, No calf tenderness
Unable to move legs, sensations intact Urine output: 400cc from the OT Pad: 3/4 soaked since from the OT
Clinical: alert and conscious, pink, hydration fair not tachypneic, not tachycardic, vitals stable and afebrile
Lungs: clear with equal air entry bilaterally CVS: DRNM PA: soft with minimal tenderness at the op site uterus well contracted at 20 weeks dressing minimally soaked
[use 20cc syringe, take 8ml MgSo4 + 12ml Normal Saline]
* use 3 way branula, give infusion while we also run Normal Saline for 15 min
Maintenance
10 ampule = 50ml MgSo4 = 25gm
[use 50cc syringe]
infusion 2cc/hr/24hr = 1g/hr
*1 ampule contain 2.47gm Mgso4
MgSo4 MOA
The mechanism of action of Magnesium sulfate in eclampsia is not clear. The postulated mechanisms are:
a. Central action: Voltage dependent blockade of NMDA (N-methyl D-aspartate) subtype of glutamate (excitatory) channel receptors
b. Peripheral action: At Neuromuscular Junction (NMJ), it causes –
Blockage of calcium entering the cell and blocking calcium at intracellular sites/membranes
Reduction of presynaptic acetylcholine (ACh) release at the endplate
Reduction of motor endplate sensitivity to acetylcholine (ACh)
Role in Severe pre-eclampsia and Eclampsia:
Magnesium sulfate is an anticonvulsant rather than an anti-hypertensive. It prevents seizures in pre-eclampsia and doesn’t treat hypertension. In eclampsia, it is given as soon as the convulsion has ended.
It causes vasodilation, increases cerebral, uterine and renal blood flow. It decreased cerebral edema.
Monitoring Hourly for Magnesium Sulfate toxicity:
Suspend or postpone use of Magnesium sulfate, if any of the following is present: